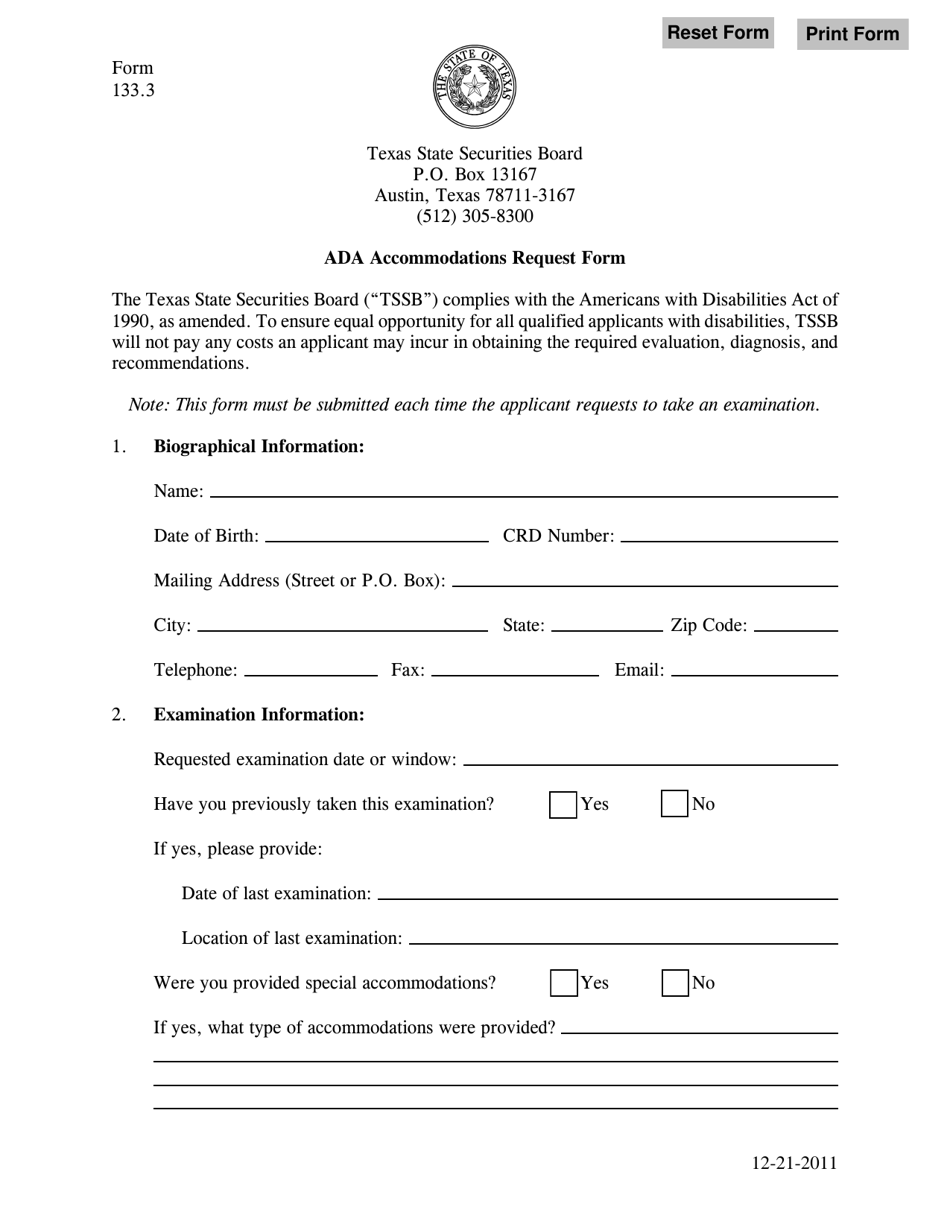
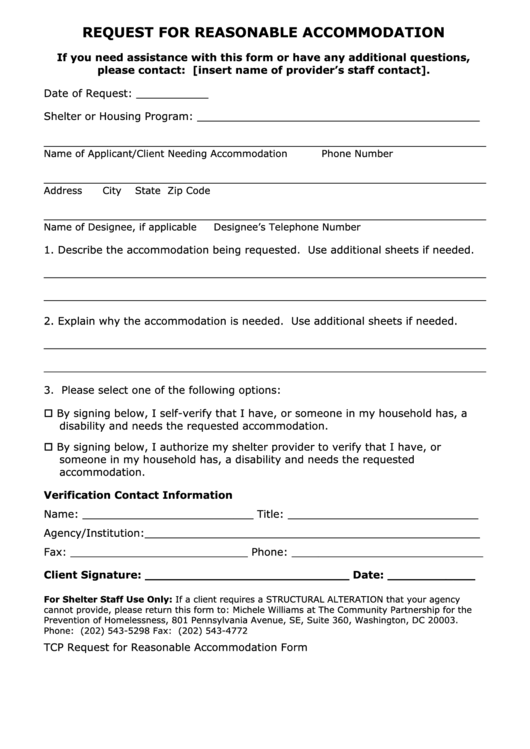
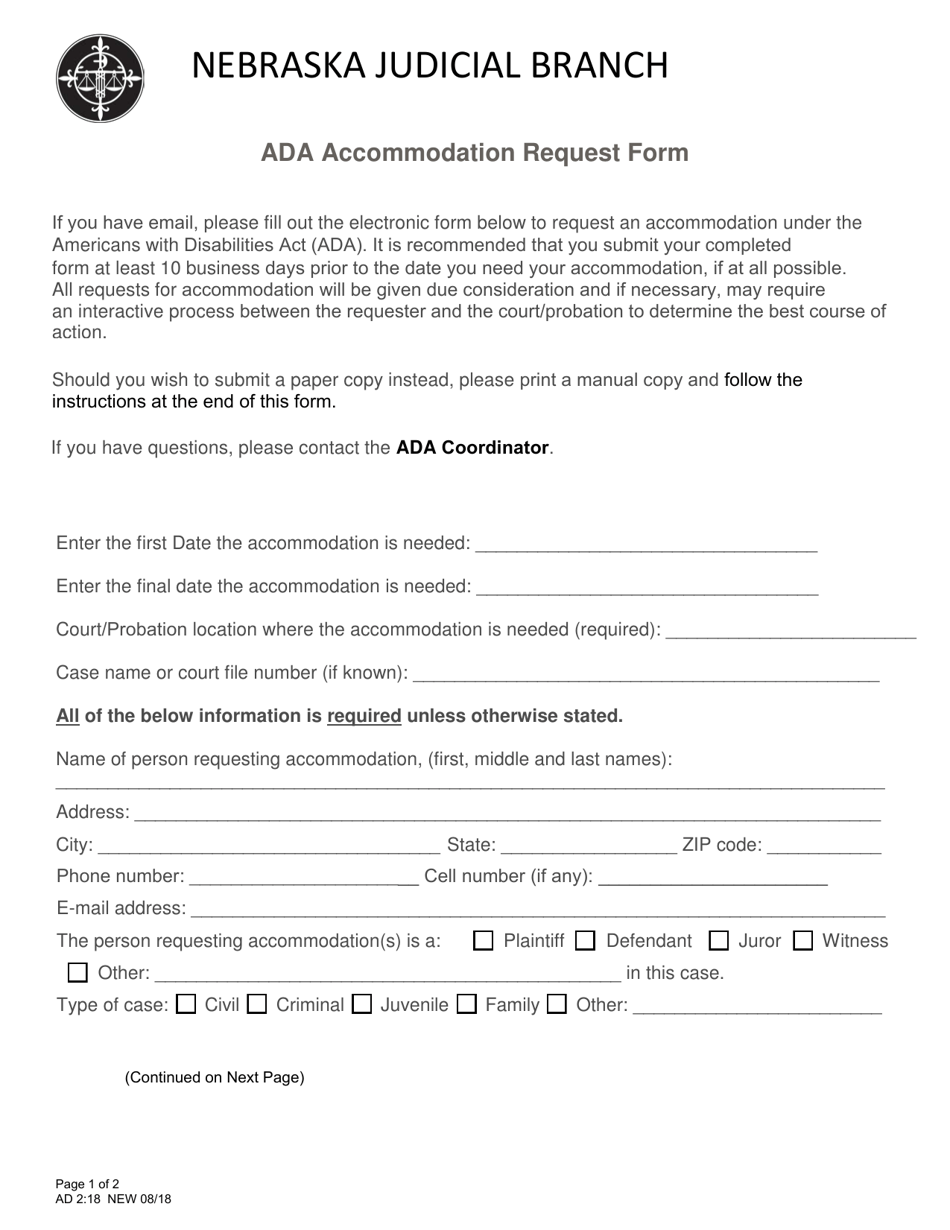
Ada Accommodation Request Form Template - Provide the name, address, telephone and fax numbers of your health care provider. The provider may receive a request from us for information. Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required for an employee.
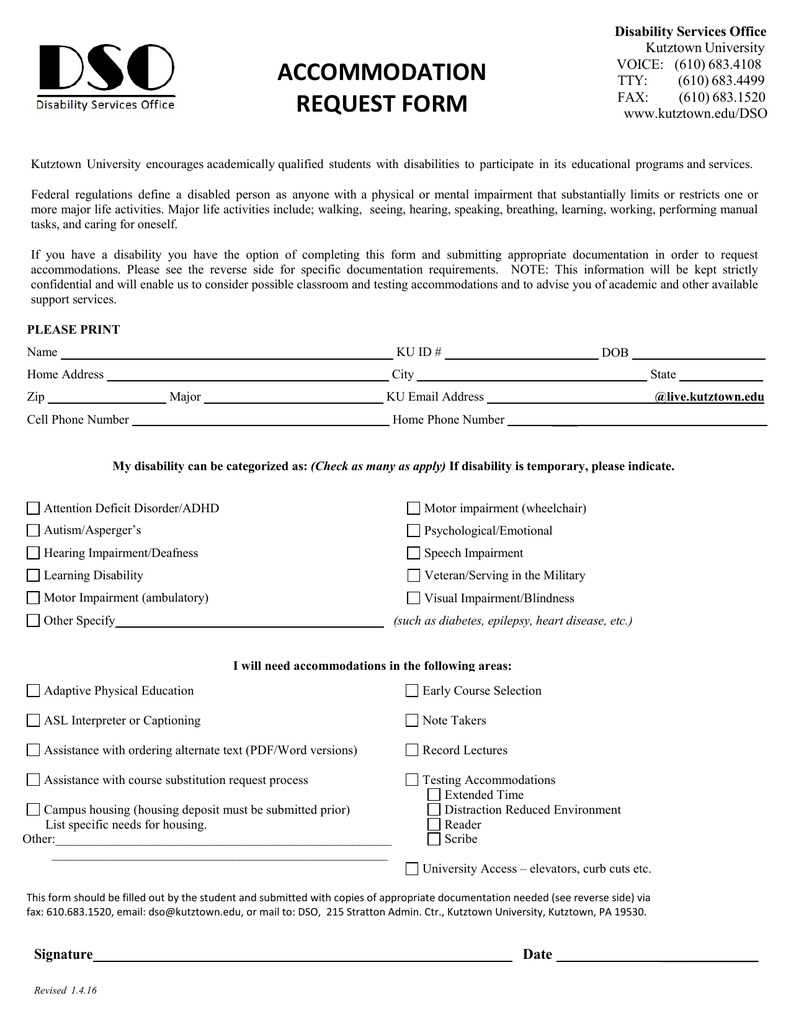
This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required for an employee. The provider may receive a request from us for information. Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. Provide the name, address, telephone and fax numbers of your health care provider.
Provide the name, address, telephone and fax numbers of your health care provider. Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. The provider may receive a request from us for information. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required for an employee.
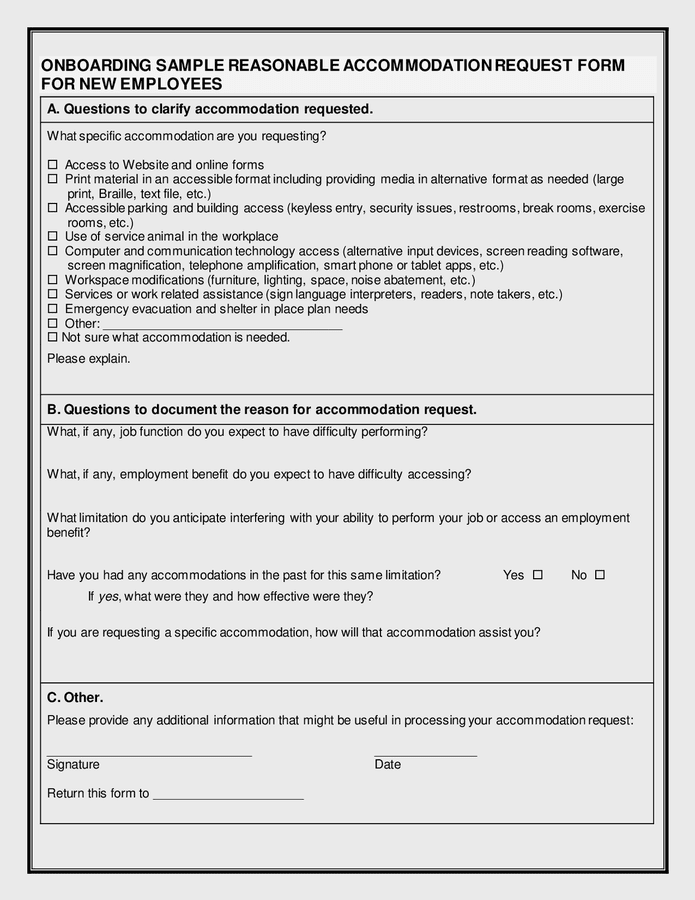
Onboarding reasonable request form in Word and Pdf formats
Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. The provider may receive a request from us for information. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required for an employee. Provide the name, address, telephone and fax numbers of.
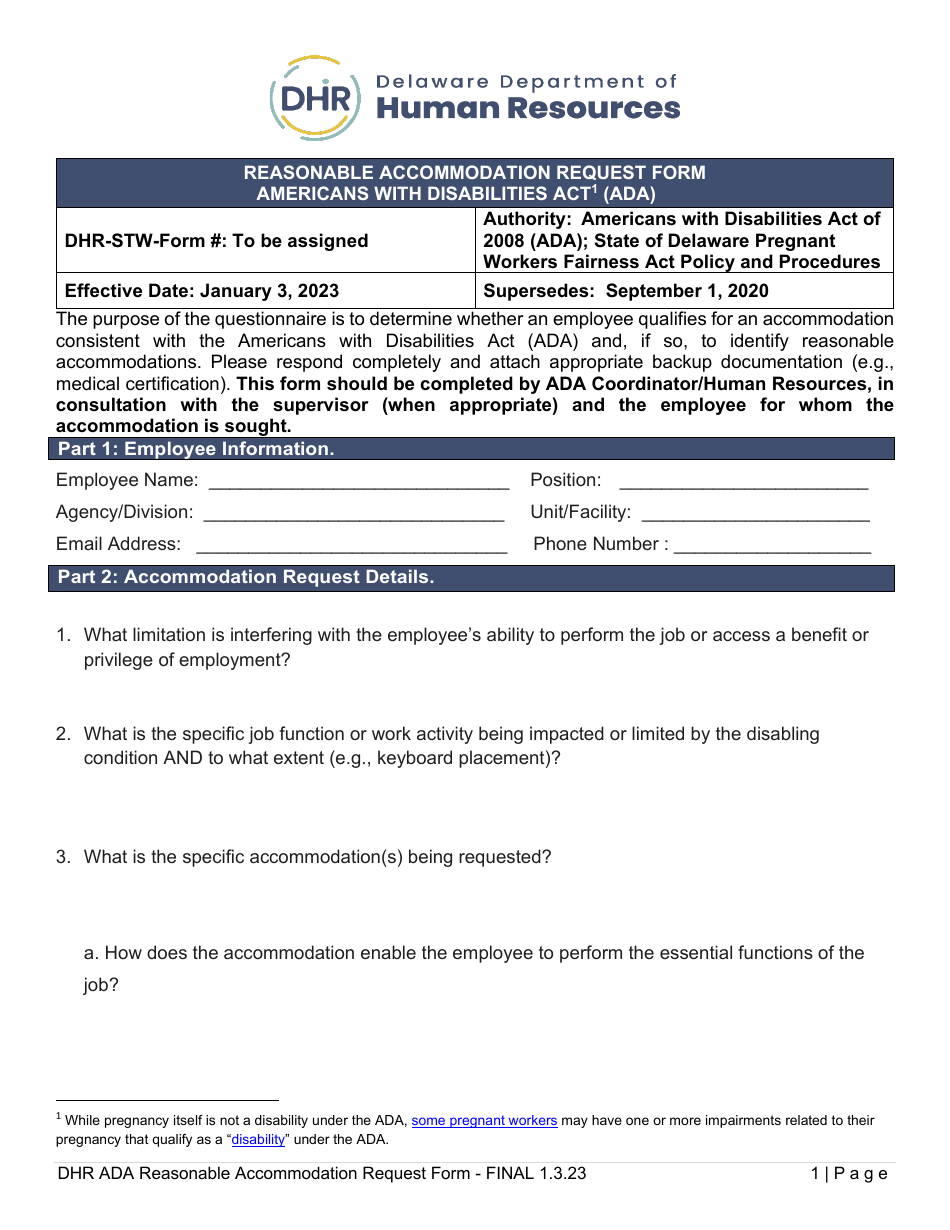
Delaware Reasonable Request Form Americans With
Provide the name, address, telephone and fax numbers of your health care provider. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required for an employee. Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. The provider may receive a request.
Ada Request Form Template
Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required for an employee. The provider may receive a request from us for information. Provide the name, address, telephone and fax numbers of.
Ada Request Form Template
The provider may receive a request from us for information. Provide the name, address, telephone and fax numbers of your health care provider. Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is.

ADA Reasonable Checklist (Free Template) AIHR
The provider may receive a request from us for information. Provide the name, address, telephone and fax numbers of your health care provider. Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is.
Reasonable Request Form Template
Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required for an employee. Provide the name, address, telephone and fax numbers of your health care provider. The provider may receive a request.
ADA reasonable request form in Word and Pdf formats
Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. The provider may receive a request from us for information. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required for an employee. Provide the name, address, telephone and fax numbers of.
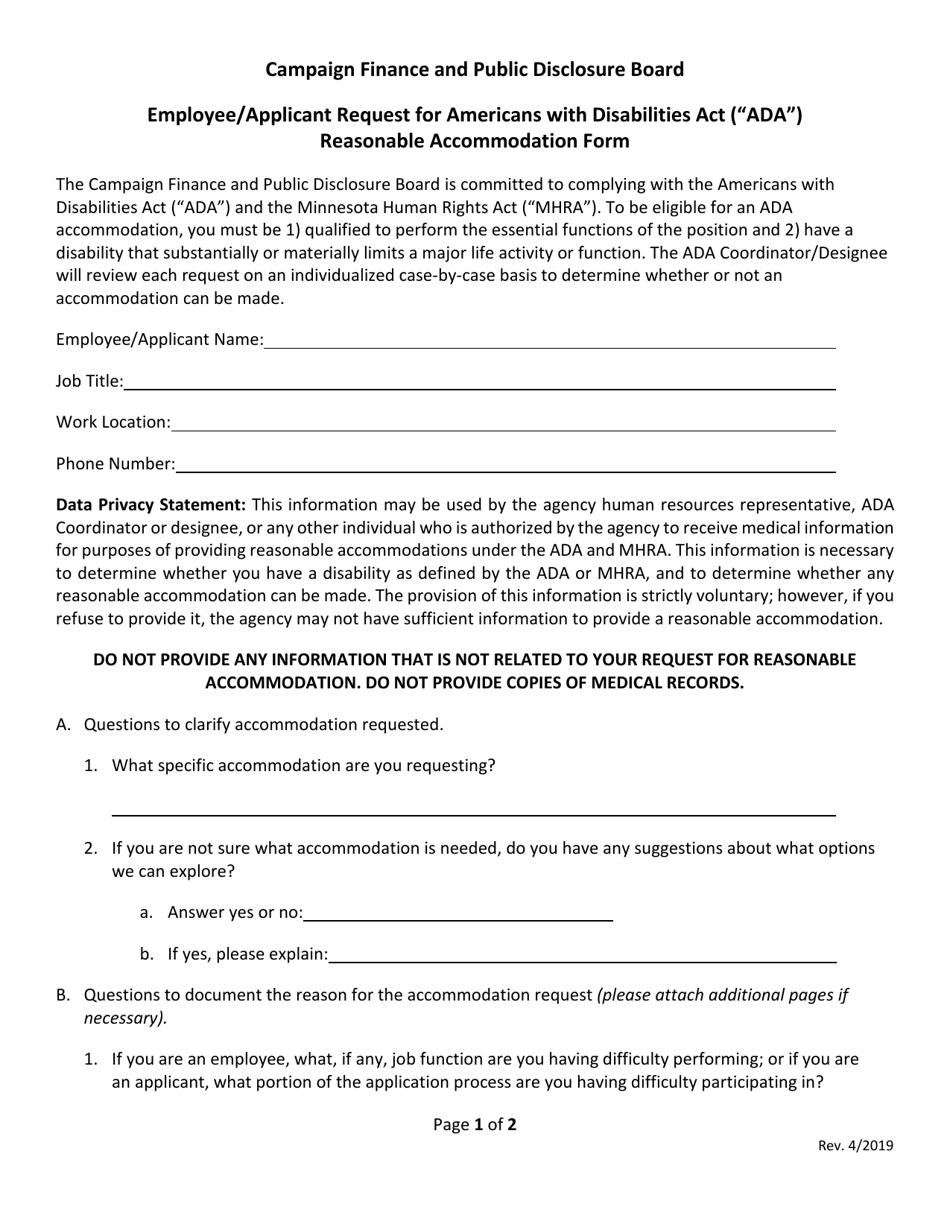
Minnesota Employee/Applicant Request for Americans With Disabilities
Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. The provider may receive a request from us for information. Provide the name, address, telephone and fax numbers of your health care provider. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is.

Recognizing an Request Under the ADA Doc Template pdfFiller
Provide the name, address, telephone and fax numbers of your health care provider. Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required for an employee. The provider may receive a request.
Ada Request Form Template
The provider may receive a request from us for information. This form is to assist the university in determining whether, or to what extent, a reasonable accommodation is required for an employee. Provide the name, address, telephone and fax numbers of your health care provider. Please complete this form to request an accommodation for a disability under the americans with.
This Form Is To Assist The University In Determining Whether, Or To What Extent, A Reasonable Accommodation Is Required For An Employee.
Please complete this form to request an accommodation for a disability under the americans with disabilities act (ada), pregnant. The provider may receive a request from us for information. Provide the name, address, telephone and fax numbers of your health care provider.