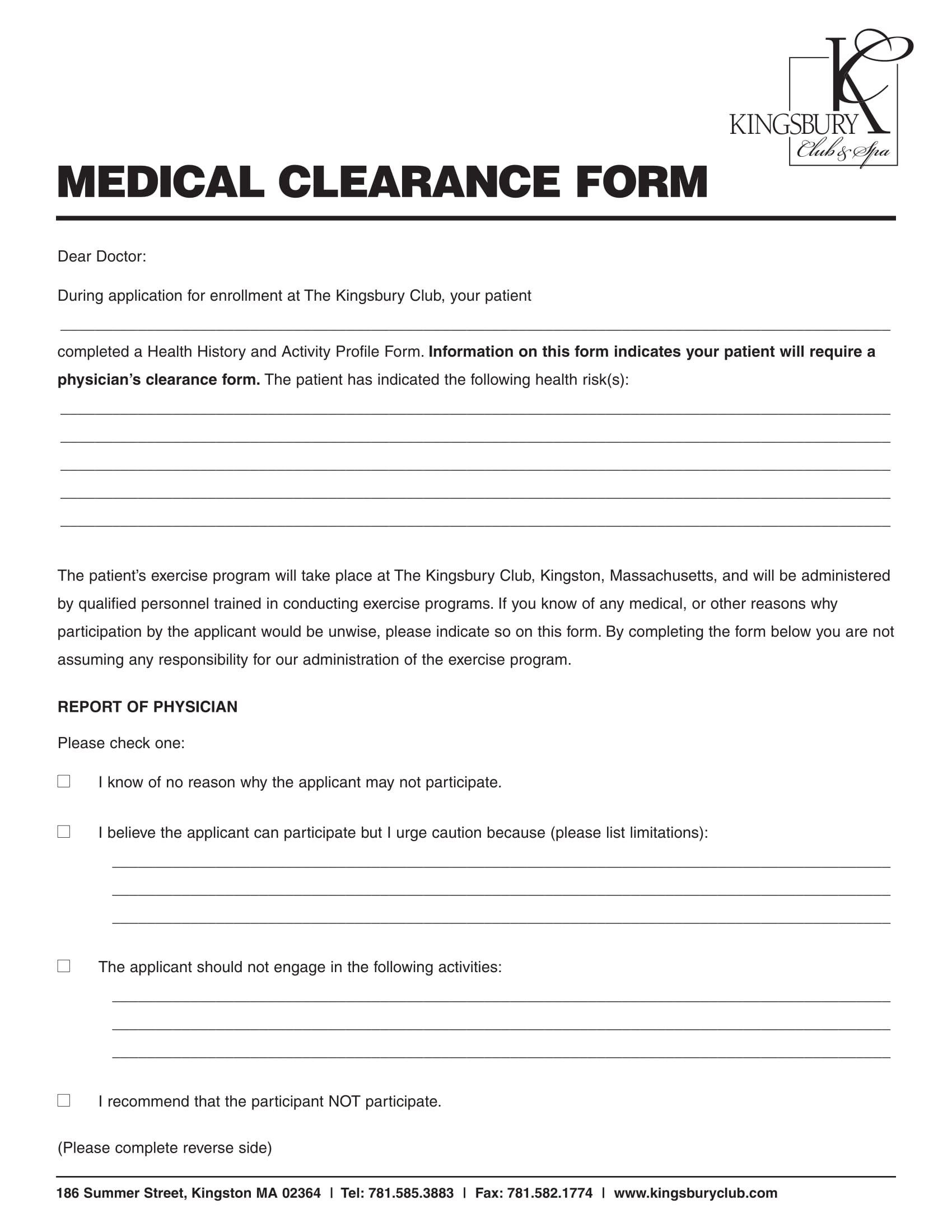
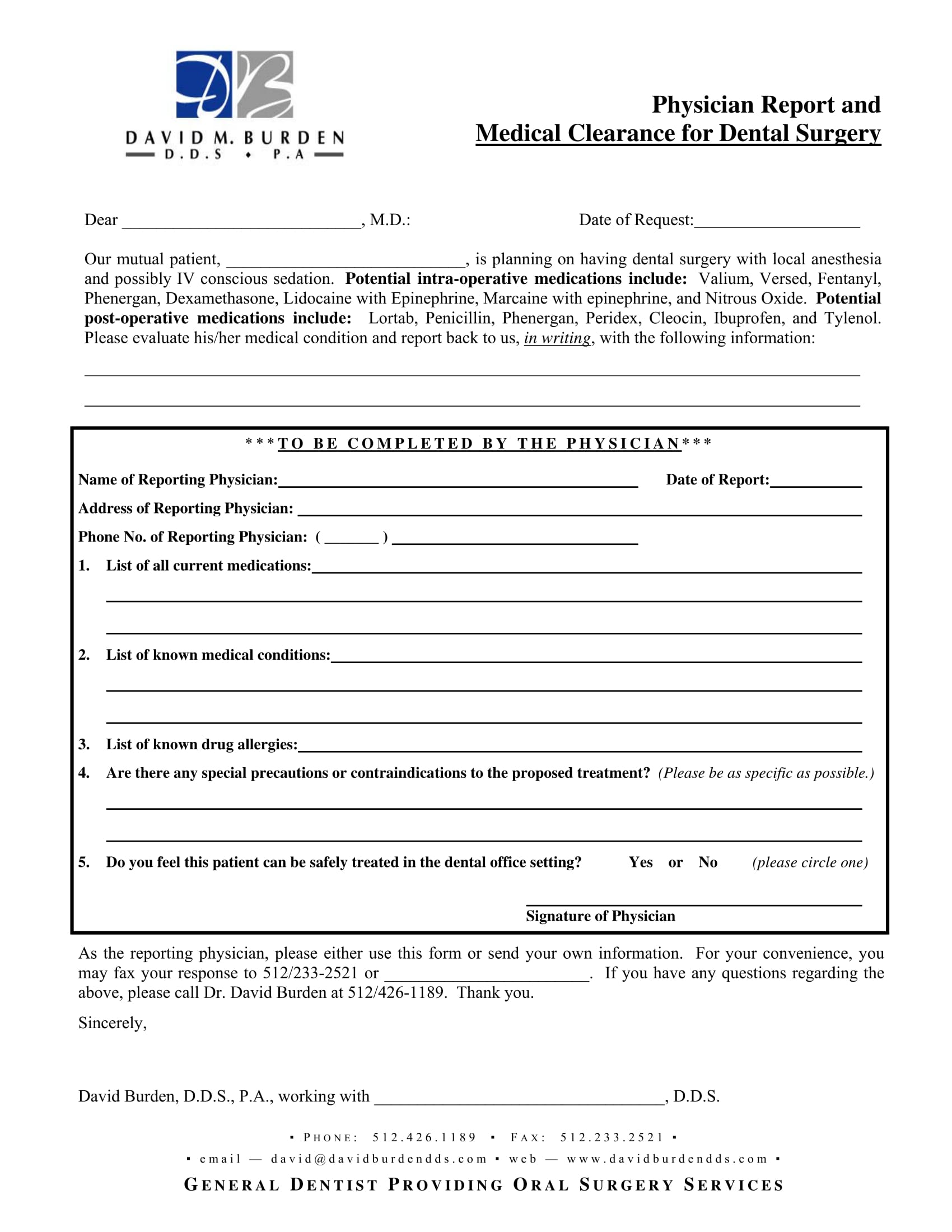
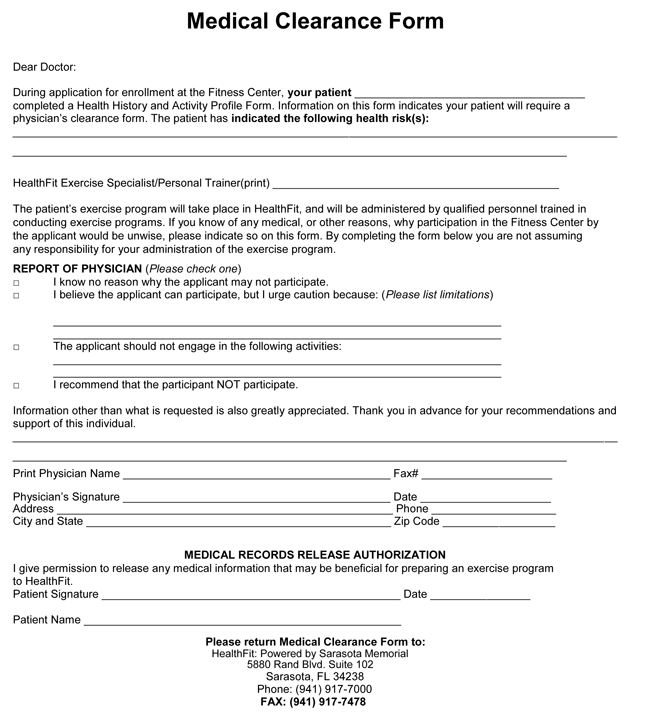
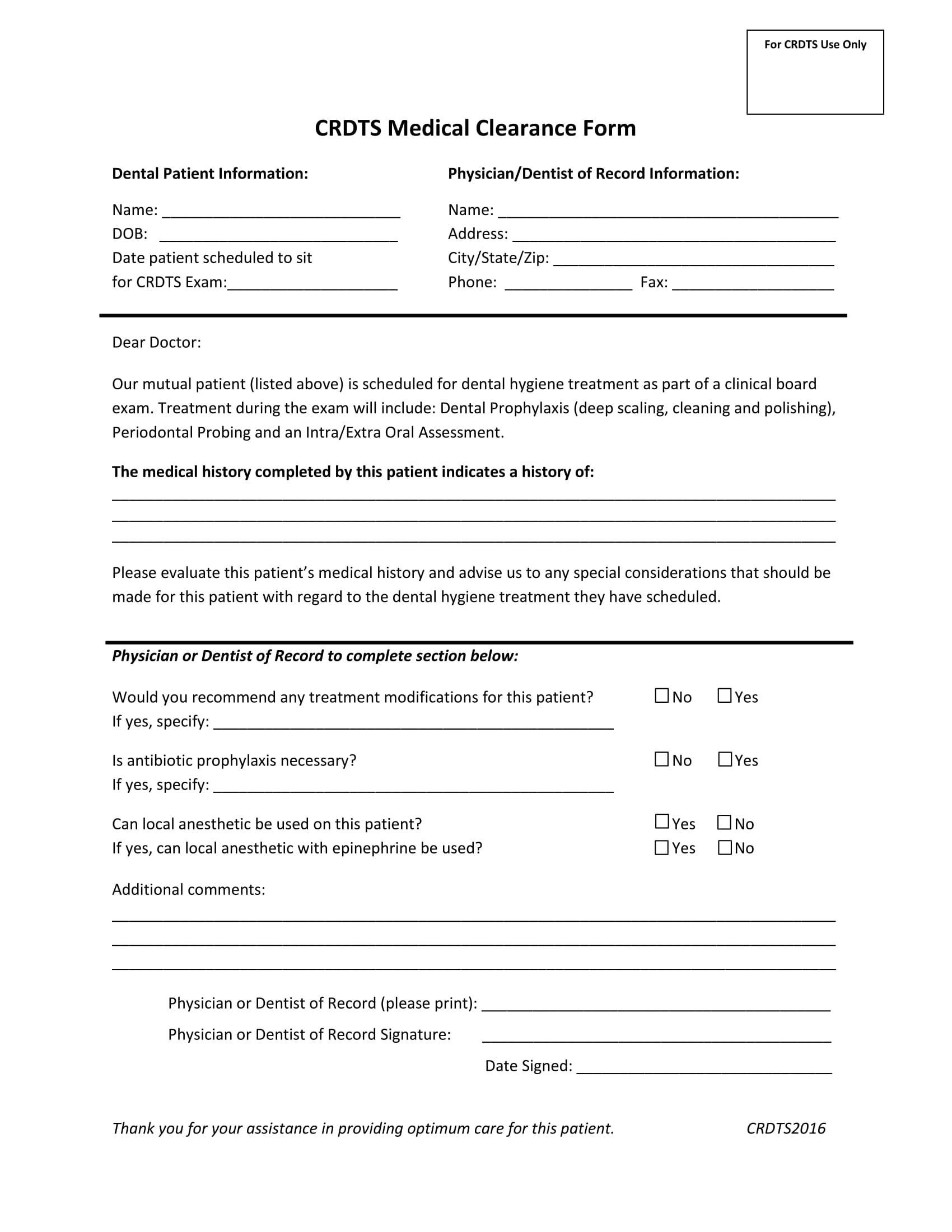
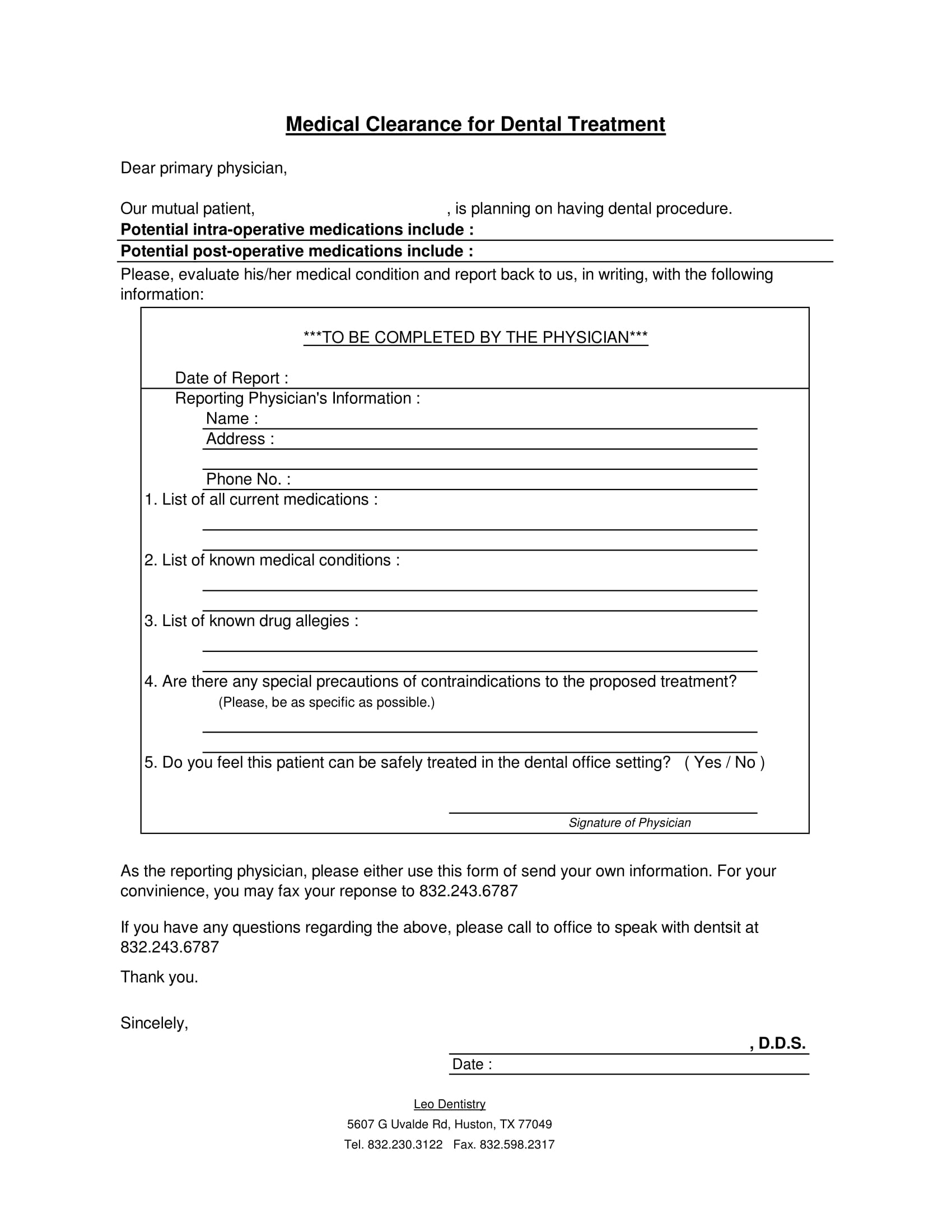
Printable Medical Clearance Form For Dental Treatment - Please provide any information regarding the above patient's need for antibiotic prophylaxis,. Medical clearance for dental treatment patient’s name:_________________________. This form is essential for obtaining medical clearance prior to dental treatment. View the medical clearance for dental treatment form in our collection of pdfs.
Please provide any information regarding the above patient's need for antibiotic prophylaxis,. View the medical clearance for dental treatment form in our collection of pdfs. Medical clearance for dental treatment patient’s name:_________________________. This form is essential for obtaining medical clearance prior to dental treatment.
Please provide any information regarding the above patient's need for antibiotic prophylaxis,. Medical clearance for dental treatment patient’s name:_________________________. View the medical clearance for dental treatment form in our collection of pdfs. This form is essential for obtaining medical clearance prior to dental treatment.
FREE 30+ Medical Clearance Form Samples in PDF MS Word
Please provide any information regarding the above patient's need for antibiotic prophylaxis,. View the medical clearance for dental treatment form in our collection of pdfs. This form is essential for obtaining medical clearance prior to dental treatment. Medical clearance for dental treatment patient’s name:_________________________.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Medical clearance for dental treatment patient’s name:_________________________. Please provide any information regarding the above patient's need for antibiotic prophylaxis,. This form is essential for obtaining medical clearance prior to dental treatment. View the medical clearance for dental treatment form in our collection of pdfs.

Printable Medical Clearance Form For Dental Treatment
Medical clearance for dental treatment patient’s name:_________________________. This form is essential for obtaining medical clearance prior to dental treatment. Please provide any information regarding the above patient's need for antibiotic prophylaxis,. View the medical clearance for dental treatment form in our collection of pdfs.
Printable Medical Clearance Form For Dental Treatment Printable Forms Free Online
Medical clearance for dental treatment patient’s name:_________________________. Please provide any information regarding the above patient's need for antibiotic prophylaxis,. This form is essential for obtaining medical clearance prior to dental treatment. View the medical clearance for dental treatment form in our collection of pdfs.

Medical Clearance For Dental Treatment Fill Online, Printable, Fillable, Blank pdfFiller
Please provide any information regarding the above patient's need for antibiotic prophylaxis,. View the medical clearance for dental treatment form in our collection of pdfs. Medical clearance for dental treatment patient’s name:_________________________. This form is essential for obtaining medical clearance prior to dental treatment.

Doctors Note for Surgery New 27 Sample Medical Clearance forms Dental treatment, Medical
This form is essential for obtaining medical clearance prior to dental treatment. Please provide any information regarding the above patient's need for antibiotic prophylaxis,. View the medical clearance for dental treatment form in our collection of pdfs. Medical clearance for dental treatment patient’s name:_________________________.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
View the medical clearance for dental treatment form in our collection of pdfs. Please provide any information regarding the above patient's need for antibiotic prophylaxis,. This form is essential for obtaining medical clearance prior to dental treatment. Medical clearance for dental treatment patient’s name:_________________________.

Printable Dental Clearance Form For Surgery
Please provide any information regarding the above patient's need for antibiotic prophylaxis,. This form is essential for obtaining medical clearance prior to dental treatment. View the medical clearance for dental treatment form in our collection of pdfs. Medical clearance for dental treatment patient’s name:_________________________.
FREE 30+ Medical Clearance Forms in PDF MS Word
This form is essential for obtaining medical clearance prior to dental treatment. Medical clearance for dental treatment patient’s name:_________________________. Please provide any information regarding the above patient's need for antibiotic prophylaxis,. View the medical clearance for dental treatment form in our collection of pdfs.

Printable Medical Clearance Form For Dental Treatment
Medical clearance for dental treatment patient’s name:_________________________. Please provide any information regarding the above patient's need for antibiotic prophylaxis,. This form is essential for obtaining medical clearance prior to dental treatment. View the medical clearance for dental treatment form in our collection of pdfs.
Please Provide Any Information Regarding The Above Patient's Need For Antibiotic Prophylaxis,.
View the medical clearance for dental treatment form in our collection of pdfs. This form is essential for obtaining medical clearance prior to dental treatment. Medical clearance for dental treatment patient’s name:_________________________.